
Healing the “Incurable” With a Simple DIY Spray Protocol & Testimonies
Visual testimonies and step‑by‑step guide for the skin protocol

Note: This is for educational purposes. This is not medical advice, and I am not telling you what you should do. Every person is or should be in control of their own health in spite of what the current medical establishment would like you to believe.
In this article, we will first review the methods for making a simple chlorine dioxide spray, look at different diseases and conditions that can be helped, and look at some of the known and theoretical mechanisms of action that explain how so many variations of diseases and conditions can be helped using the spray/topical protocol.
The Simple Spray Protocol:
For superficial wounds (e.g., small cuts, insect stings, and bites), skin conditions (e.g., psoriasis, eczema, and dermatitis), and infections (e.g., impetigo, athlete’s foot, and ringworm)
Step 1:
Add 10 activated drops of MMS (MMS1) to 1 ounce (30 ml) of water**
See previous post to understand basic activation of MMS
**Only use filtered, reverse osmosis, or distilled water.
Step 2:
Spray on affected area at least three times per day. After spraying, let the area air dry. Do not cover with a bandage until air-dry.
Notes:
Always follow the three golden rules and adhere to the low and slow principle discussed in a previous post. Link to previous post HERE.
In my experience, it is wise to start with a weaker solution, like five activated drops in 30 mL of water, to ensure that your skin is not sensitive.
Do not use tap water for any MMS mixture, as it is not safe to risk getting impurities in the solution. Use only bottled drinking water, reverse osmosis, or distilled water.
In most places, 2-ounce or 4-ounce size spray bottles are available at the pharmacy or in health food stores. Food or medical grade plastic is okay for the diluted solution. Glass is also acceptable. I prefer using a 2-4 ounce spray bottle since I replace the solution every week or two.
If a smaller or larger volume is needed, use this reference:
2 drops MMS1 to 1/4 oz (10 ml) of water
5 drops MMS1 to 1/2 oz (15 ml) of water
10 drops MMS1 to 1 oz (30 ml) of water
15 drops MMS1 to 1.5 oz (45 ml) of water
20 drops MMS1 to 2 oz (60 ml) of water
30 drops MMS1 to 2.5 oz (75 ml) of water
40 drops of MMS1 to 4 oz (80 ml) of water
It is better to keep the solution in the refrigerator if possible, as this will prevent the Chlorine Dioxide from evaporating out of the solution.
In general, this mixture will last up to a week if not refrigerated. It will last 2-3 weeks if refrigerated. You will know that it has lost its potency when the original color begins to noticeably fade.
Deep Wound Protocol:
For very severe wounds and ulcers that reach into and below the dermis, it is best to use a solution of hyperpure chlorine dioxide known as CDS (Chlorine Dioxide Solution). Hyperpure CDS can be purchased online, and it can also be produced at home using the drops we have been discussing and distilled water. Here is a video that demonstrates the home production of hyperpure CDS. This protocol for topical use using CDS is referred to by many as protocol D. The D stands for dermatological.
Direct link to Video: https://rumble.com/vm5qff-training-video-2-cds-history-and-demonstration-making-concentrated-cds-3000.html
Protocol D (Dermatological)
Standard Concentration
When produced at home or purchased, the CDS solution will be a standard concentration of 3% chlorine dioxide (0.3% = 3000 ppm). This hyperpure solution can be lightly sprayed on the skin and in wounds. Often, this concentrated solution is referred to as CDS-3000.
Application
1. Fill a spray bottle with CDS 0.3% (3000 ppm).
2. Lightly spray to fully expose the affected area to the ClO2.
3. The solution should be lightly sprayed so the CDS does not pool in deep wounds or on tissues.
4. Allow the lightly sprayed area to air dry before applying any kind of dressing.
The CDS should not cause burning or stinging. If it does, dilute the solution by half.
The spray application can be repeated several times a day or even every hour if desired, until full healing is achieved.
This protocol can be used also in replace if the Simple Spray Protocol if desired.
Precautions:
Do not use occlusive bandages with the concentrated solution.
The solution should not be allowed to pool in a wound or region of the body like the navel for more than a few minutes, as this can result in a burn.
If the spray spring shows signs of rust/corrosion, the sprayer should be replaced.
Notes:
If you do not want to make your own CDS 3000, you may be able to find CDS 3000 at one of the following websites.
USA Suppliers:
https://waterpureworld.com/
https://onenesslabs.com/
https://kvlab.com/
Worldwide supplier list:
https://t.me/mmsCDSlinks (telegram app needed to open this)
Here are a couple of examples of what the CDS 3000 product will look like.


Spray Protocol Testimonials And Mechanisms of Action
The testimonials reviewed here are not comprehensive, but I have chosen these testimonials because the people who sent them to me were thoughtful enough to take pictures before, during, and after, and this makes reporting and documentation much easier. As they say, “a picture is worth 1,000 words.” There are a few testimonials that do not provide pictures due to the sensitive nature and location of the problems.
WARNING: Some of the images in this article show open wounds, and if you have a weak stomach, you have been forewarned. All of these testimonials were provided by people who used topical chlorine dioxide protocol in the treatment of a skin disease/condition, and in some cases they used multiple protocols
Skin Infections
Chlorine dioxide as an antimicrobial agent acts primarily through oxidation, disrupting the cell walls and membranes of microorganisms, leading to cell lysis and death. It is a strong oxidizing agent that can denature proteins and inactivate nucleic acids, thereby preventing microbial replication and survival. [1, 2, 3] The oxidative stress induced by ClO₂ is effective against a broad spectrum of pathogens, including bacteria, viruses, and fungi.
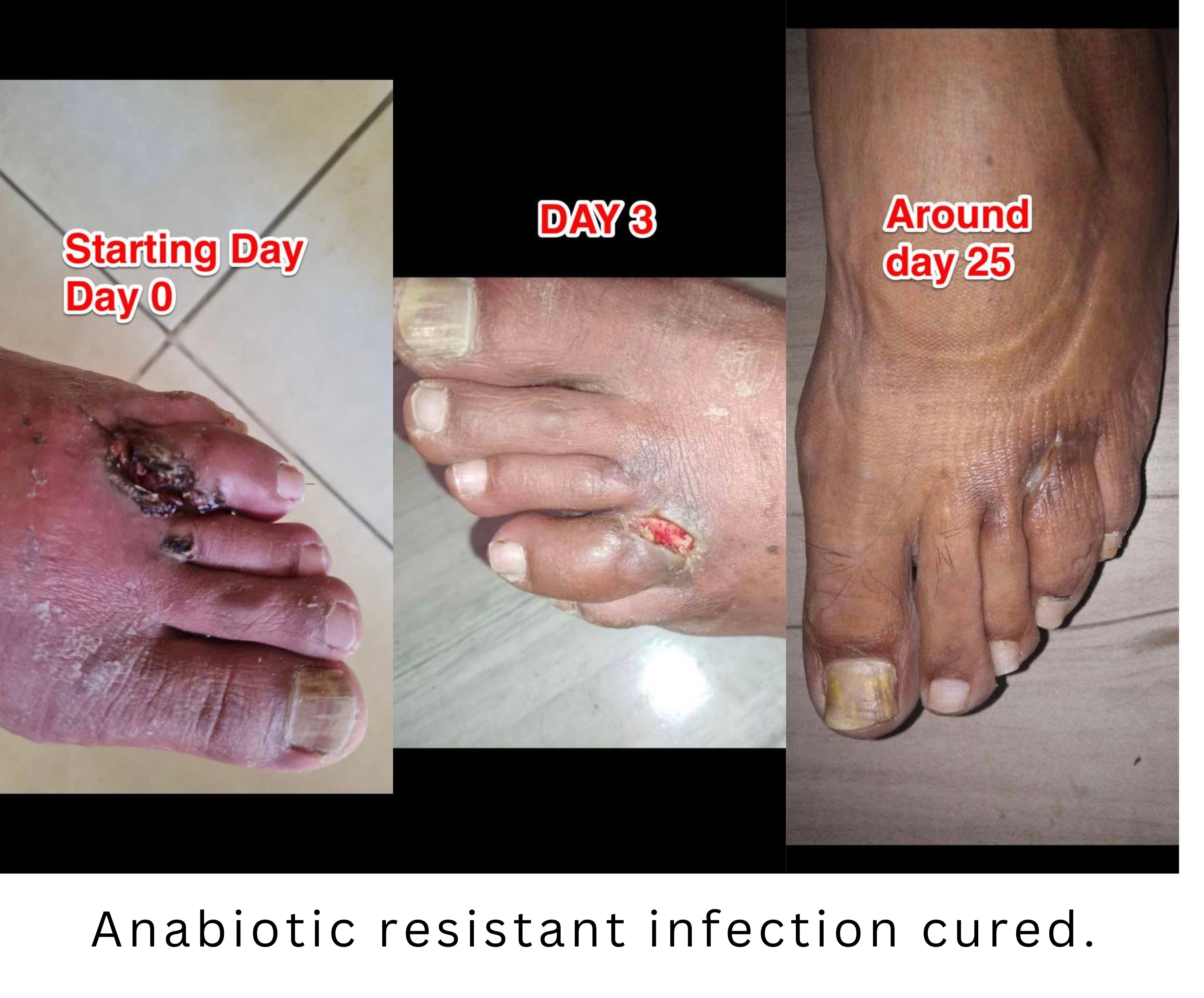
Testimonial: Antibiotic Resistant Infection

“My son had an infection in his left arm. He was away from home and went to an urgent care where they gave him IV antibiotics. These pictures are after the IV- unfortunately I don’t have the original pic was also great swelling. By the time I finally saw him the arm was in this state below- A Strange bump in the vein as well as these open sores. Remember this is AFTER IV antibiotic and I did NOT want him getting more drugs.
We started with the CDS solution prepared according to The Curious Outlier’s instructions - a stock solution- the only difference I did was I made it in 16oz- not the recommended 24 oz. We did 12 drops of Part A and then 18 drops of the HCL (part B).
He drank it every hour most of the day and we also sprayed it on the skin regularly. I put this mixture of the CDS in a 2oz spray bottle as well as 2-4 drips of 70% DMSO.
Right away the arm changed. We stayed with this program for 5 days - but it had looked cleared up after 3 days.
OriginalTestimonial Source Link
Testimonial: Severe Leg Infection

(Translated from Spanish)
“I’ll tell you a case that luckily I was able to help with CDS and DMSO. I’m attaching photos. They were going to amputate his leg, and I told him first why he doesn’t try CDS and DMSO and then go to the doctor. After a month of using it, he sprayed CDS on the wound and put it where the veins and arteries pass (since they were obstructed) which was the reason for the amputation. CDS + DMSO + CDS. When he went to have it redone, his arteries and veins were clean and his leg was intact. The first photos were when he left the hospital, the last photo is after 30 days of the application.”
2nd message:
“In addition to that, he could not move his legs and arms and taking DMSO a few times, about 15 drops in a glass of water, he began to move them.”
3rd message:
“It may have been a stroke and taking it quickly did not affect him. That was the day before he started using using the CDS and DMSO on his legs.”
Link to original source message.
Testimonial: Staphylococcus Aureus and Enterobacter Skin Infection
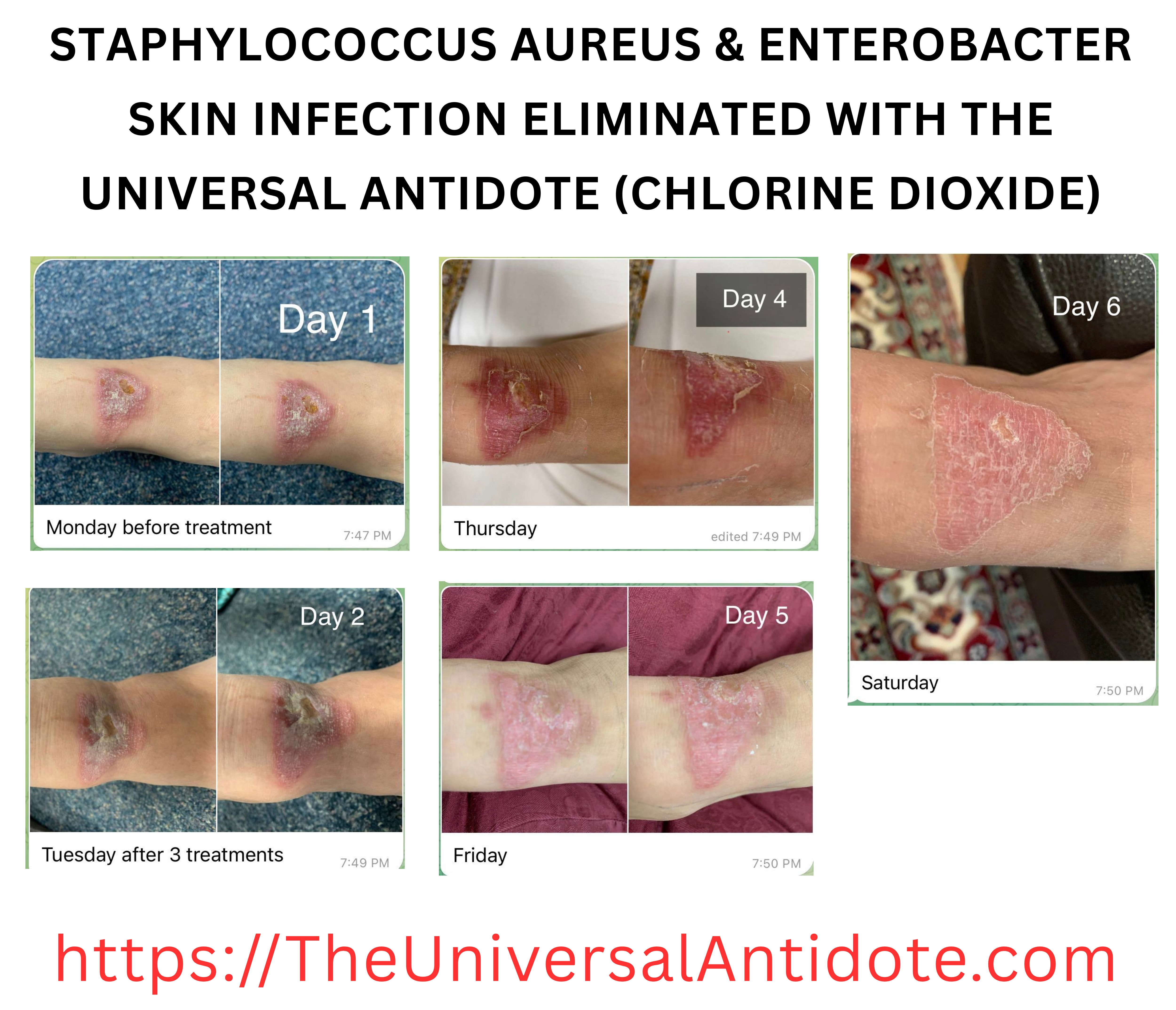
This skin infection was treated with a different protocol they used a modified Gas Protocol, but the spray protocol would have worked efficiently for this as well.
This testimonial was received through a private message, so no source link to an original message is available
This infection was treated with the bag protocol by wrapping the ankle in a medium sized bag. Placing a small mason jar in the bag. With 10 activated drops in it. Sealing the bag and left in place for 5 min. Repeated every four hours three times in one day. There were no more treatments after that, but if it was me, I would’ve treated for several days to ensure for elimination of the infection.
Testimonial: Antibiotic Resistant Leg Wound Infection

“My next door neighbor was hospitalized because a truck ran into his work house and a wall fell on him. He had a savage wound to his lower leg above the ankle that got infected. Doctors gave up trying to heal it and told him they believe the leg should be amputated below the knee. My son took him a strong batch, 10 drops per ounce, of CDS in a 3 ounce spray bottle from Walgreens and instructed him not to let the doctors know. It healed, the doctors were shocked, and when he showed him what he was using, they didn’t want to know. I have incredible before and after pictures. Does anyone know how I can get these to an admin to maybe post them?”
In a private message the person that shared the testimonial gave me more information and the pics.
“In the gross picture, he had already been hospitalized 4 or 5 weeks. They gave him tons of intravenous antibiotics but nothing worked. His doctors told him at that point they felt they needed to amputate his leg to prevent a gangrene type infection from developing and spreading... That is the point at which I learned of his injury from my son. We sent him a spray bottle of CDS which his wife snuck into the hospital. It only took about 4 weeks or so from that point for it to heal completely. He told me that within the first 2 days he knew it was healing.”
Original testimonial source message
Testimonial: Infected Dog Bite

PHYSICIAN REPORT
(Translated from French)
“A 12-year-old child bitten by a stray dog on the anterior inner side of the left thigh, causing a wound with loss of tissue.
He presented to my consultation after 3 days with necrotic areas and a secondary infection.
I applied pure CDS to him by spraying 10 cc on a compress every 15 minutes for 4 hours.
After the disappearance of the superinfection, on day 4 from the start of treatment, I opted for a suture in the middle of the wound in order to bring the edges together.
I continued to spray pure CDS on the wound, 6 hours a day, keeping the child in the observation room, he left to make these compositions, which lasted 5 days, and returned to my house to continue the protocol.
The wound completely healed after 21 days of treatment, just with skin applications of CDS 😊
Dr Djamila Ghiar”
Link to original source testimony
Testimonial : Unknown Bacterial or Fungal Infection

First picture is before treatment began and the second image is about 20 days after starting the treatment. The third image was at about 40 days.
This person started with both oral consumption and topical spray of activated MMS. Oral consumption started with 1 activated drop four times a day and then ramped up over several days to taking 4 activated drops 4 times per day.
The spray concentration is not known, but they said it was a weak solution and so I am assuming it’s between 50–100 ppm spray. The spray was being applied twice per day.
Protocols used:
I received this testimonial in a private message, so I do not have a link to an original testimonial.
Testimonial: Severe Burn and Infection

“My husband was diagnosed as type 2 diabetic back around 2007. He didn’t take care of himself. After he got a foot wound it became infected and he got gangrene, then a partial leg amputation in 2016. He started getting insulin. In 2020 I began green juicing it seem to balance his sugar and the doctor took him off insulin. Prior to that, around September 2019 he went to the ER due to hemorrhaging behind his eyes later declared legally blind due to severe retinopathy. He was told he had stage 2 kidney disease. While in the hospital the doctor gave him a heart burn med called Omeprazole. A few months later when he was filling up with fluid it was documented that that med caused him to go into Stage 5 renal failure. He had also been dealing with some neuropathy which had gotten worse by 2022. From the a little below the knees down to all his foot, he felt nothing. I’m going to fast forward to Christmas 2022. My husband pulled up close to him a portable heater I had recently put out. I was not with him but was with his mom that had been visiting. When I came to the bathroom where he was his leg was badly blistered. I was in such shock I didn’t think of taking a picture. He did not feel any pain. I began spraying his burn wound with mms several times a day and soaking his foot in it. I also checked all his vitals and they remained in his normal range. I immediately gave him diluted oregano oil under his tongue 2x a day to keep infection away. I will share some pictures. It is still healing but it is so much better.
Link to original source message
Testimonial: Severe Foot Infection
(Translated from Spanish)
“Testimony of persistent infection in a toe that was practically severed by a motorcycle accident and with a severe internal bone fracture. After more 45 days after of taking antibiotics and disinfecting as indicated by a doctor, the toe was getting worse and worse and even had a foul odor, seriously fearing the worst. They couldn’t get the stitches out because of how bad that infection was.
Photo 1: Chlorine dioxide in pure spray 3 times a day with deep cleaning each time and once it dried, a cream that a new doctor prescribed was added.
Photo 2: After 3 days, the changes were more than significant, noting that the tissue was already beginning to regenerate from within.
Photo 3: After 3-4 weeks of treatment.
Testimonial: Severe burn and infection

This is a testimonial This is a physician report. This patient was treated during the pandemic after he was in a house fire and while escaping the house, he ran across a floor that was on fire. He is a diabetic and subsequently developed a severe infection in the burns that he had on his feet.
Clinical Case Report
Age: 48 years
Sex: Male
Relevant medical history:
A patient with a diagnosis of type 1 diabetes mellitus, presenting with chronic non-healing wounds, refractory to previously applied conventional therapeutic approaches.
Follow-up period: 2 months.
⸻
Therapeutic Intervention
A comprehensive therapeutic protocol was implemented, integrating nutritional management and adjunctive topical and systemic interventions, as detailed below.
Nutritional management
An alkaline-oriented dietary approach was implemented with the objectives of:
Reducing systemic inflammatory burden.
Promoting a metabolic milieu conducive to tissue repair and regeneration.
Supporting acid–base balance in the context of chronic metabolic disease.
⸻
Chlorine dioxide (CDS) – Systemic administration
Chlorine dioxide was administered orally according to the following protocol:
Preparation and dilution: 10 ml of chlorine dioxide solution (CDS) diluted in 1 liter of water.
Administration schedule: The solution was consumed in divided doses throughout the day.
Therapeutic rationale (descriptive):
Systemic administration was intended to support redox homeostasis, potentially enhance tissue oxygenation, and accompany reparative processes in a patient with type 1 diabetes mellitus and chronic, poorly healing wounds.
⸻
Chlorine dioxide (CDS) – Topical application
As an adjunctive local intervention, chlorine dioxide was applied directly to the cutaneous lesions:
Preparation and dilution:
50% water / 50% chlorine dioxide solution (CDS).
Application frequency:
Twice daily application to both wounds.
Testimonial: Incurable Canine Oral Papilloma Virus

After 6 months of uncontrollable growth of the pappilomas and the veterinarian giving up on the dog, she is cured.
Here’s what they did:
1 Activated MMS drop 3x/day in her mouth with 10ml water (approx 1 Tbl) and then more drinking water after, with CDS 3000 ppm full undiluted spray directly on the external and gum-line growths 5x/day, and 1 Tbl Activated MMS in a full bath for 20 minutes 3x/week.
Link to original source message
Diabetic Ulcers and Non-Healing Wounds
Diabetic foot ulcers remain one of the most devastating and costly complications of diabetes, often culminating in limb amputation and a mortality rate rivaling many cancers. Despite advances in standard care, off‑loading, revascularization, antibiotics, and meticulous wound management, far too many ulcers still fail to heal, suggesting that current approaches do not adequately address the underlying metabolic, vascular, immunologic, and infectious drivers of this condition. Chlorine dioxide and its chlorite‑based derivatives represent a low‑cost, mechanistically rich, and largely overlooked therapeutic strategy that appears to target many of these pathways at once, with early clinical studies and anecdotal accounts, reporting robust improvements in wound healing.
There are multiple proposed mechanisms of action involved in the response of diabetic non-healing ulcers to chlorine dioxide.
Improved glucose control
In small clinical studies, chlorite (particularly as WF10) lowered hemoglobin A1c and fasting glucose in people with long‑standing diabetes and severe foot ulcers. Better glucose control reduces oxidative stress and inflammation in blood vessels and nerves, creating a metabolic environment that is far more compatible with healing instead of chronic breakdown. [4, 5]
Improved vasculopathy and oxygenation
Chlorite appears to rebalance reactive oxygen species by decreasing harmful superoxide while maintaining hydrogen peroxide at levels that support vessel health and new capillary growth. This shift, along with increased tissue oxygen tension, helps reopen the compromised microcirculation in diabetic limbs, delivering the oxygen and nutrients that chronic ulcers desperately need. [4, 5]
Slowing progression of neuropathy
Diabetic neuropathy is driven by high glucose and oxidative damage to nerves and their microvasculature. By improving glycemic control and small‑vessel blood flow, chlorine dioxide–derived chlorite may indirectly protect neurons, reducing the risk of painless injuries that progress into deep, non‑healing ulcers. [4, 5]
Anti‑inflammatory immune modulation
Chlorine dioxide and chlorite act as redox‑active immune modulators that can quiet chronic, destructive inflammation without shutting down host defense. They inhibit overactive neutrophil migration, shift macrophages from pro‑inflammatory M1 to healing‑oriented M2 phenotypes, and generate taurine chloramine, which promotes resolution of inflammation in stubborn wounds. [4, 5]
Antimicrobial and anti‑infective effects
Chlorine dioxide is a selective oxidant that damages microbial proteins, membranes, and genetic material, causing rapid death of bacteria, viruses, and fungi. In clinical work with WF10, this broad‑spectrum activity translated into lower infection scores and less necrotic tissue in diabetic foot ulcers, reducing one of the main barriers to healing. [4, 5]
Direct wound‑healing and antioxidant support
Topical chlorine dioxide gels and chlorite‑based formulations have accelerated wound closure, increased granulation tissue, and enhanced collagen and capillary growth in animal models and human studies. These treatments upregulate key antioxidant enzymes like superoxide dismutase and glutathione peroxidase in the wound bed, protecting regenerating tissue from oxidative injury. [4, 5]
Synergistic, systems‑level action
Viewed together, these mechanisms suggest a single therapeutic strategy that simultaneously improves glucose control, restores microcirculation, recalibrates oxidative stress, calms inflammation, controls infection, and directly supports tissue repair. This multi‑level synergy offers a compelling explanation for the remarkable limb‑saving responses reported in early case series and small trials, and strongly justifies rigorous, larger randomized studies to confirm and refine these findings. [4, 5]
Testimonial: Heel Ulcer




“…I can relate somewhat, I had to secretly spray cds on my dad’s foot ulcer in hospital when no one was looking. I sprayed every hour 6 times a day for about 4 weeks straight. Also gave my dad cds orally and by the 5th week my dad’s non-healing ulcer that he has had for 7+ years was finally all healed up. I have a more detailed post about this on the other channel.”
“No my dad did not have diabetes. What he had was osteomyelitis (i.e. bone infection) which did not allow his foot wound to heal. Well that’s how the doctors explained it to us.”
“I don’t have the exact dates, we didn’t start taking photos until about a week into the treatment.”
“One of the photos was from my sister’s phone, the last photo of the foot fully healed was from the podiatrist. If I had to guess, I would say they are about a week apart.”
Testimonial: Non-healing, diabetic foot ulcer and neurology

This woman had a foot ulcer that was ready for amputation. She started using Colloidal Silver for the first week but then switched to CDS thereafter.
CDS was sprayed on the diabetic for ulcer and taken orally.
Note that she had no feeling in her foot due to neuropathy, however after two months of CDS she could feel pain again as she bent her toes. The pain she felt was a good sign that her neuropathy was healing as she also healed her diabetic foot ulcer.
I do not have the original source message for this testimonial.
Testimonial: Non-healing diabetic foot ulcer

(Translated from Italian)
“Taking 20 ml in a liter of water every day in 8 doses (Protocol C) and washing the wound well and applying DMSO diluted to 70% in a spray, that is, 7 ml of DMSO and 3 ml of water, wait about 30 seconds or a minute and also apply in a spray. CDS3000 (Protocol D)”
Testimonial: Non-Healing Toe Ulcer

My 86 year old grandmother’s toe had necrosis for 8 months. They tried different creams and medicines on her toe, but nothing worked.
It was healed after using Chlorine Dioxide and DMSO together for 2 months.”
Testimonial: 2-Year Old Non-Healing Leg Ulcer

“My mother-in-law, with a leg ulcer for more than two years, with antibiotics, creams and nothing cured it. I gave her a spray with CDS and told her to lie down as many times as she could. After more than a month and days she was completely healed.
Editors note:
To me, the peripheral vascular disease present in the first picture also looks much better in the second.
Testimonial: Necrotic Leg Injury Healed

Testimony of the woman that helped this man (Gladis Alvarado)
(Translated from Spanish)
“My father-in-law is 79 years old, hypertensive, has rheumatoid arthritis, and peripheral venous insufficiency. He had an accident with his truck. The front tire ran over his thigh. He was standing outside his truck with the door open and he didn’t realize he had the reverse gear on. And when he turned it on he got knocked down with the door and that was how the tire passed over his leg.
He did not want his sons to take him to the hospital. So he was prescribed antibiotics and anti-inflammatories over the phone.
Obviously he needed more medical attention. But his sons say that he is quite reluctant to go to the doctor. That’s why they asked me to go see him at the ranch where he lives.
I already found him with the necrotic wound and he had the injury for about 45 days when I started helping him.
And I began with protocol D of chlorine dioxide, which consists of applying undiluted CDS 3000pm with a spray bottle to the wound 3 times a day.
I took a picture every week. It took 7 weeks to heal.”
Testimonial: Venous Stasis Ulcer
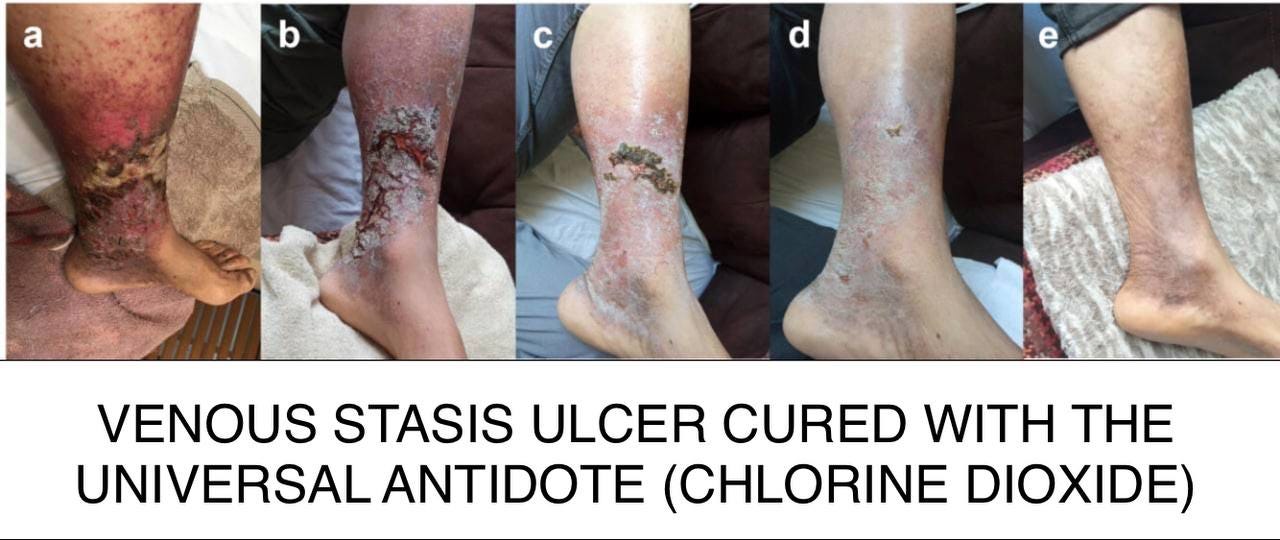
A 69-year-old man with chronic venous insufficiency:
a) lesion day 0 of treatment
b) lesion on day 5 of treatment
c) lesion on day 17
d) lesion at 28 days of treatment
e) lesion in the 2nd month
Cured in 2 months with regular application of pure CDS every 2 to 3 hours leaving in the open air.
D+ Protocol.
C20 protocol in 1 liter of water+
70% DMSO in 50ml of water divided into 3 volumes taken orally every 8 hours before each meal.
Testimonial: Circulation Restored to Ischemic Foot

(Translated from Spanish)
“The first photo from the end of May. The last photo is from the end of June, it is the progress using topical CDS. My dad is on anticoagulation and has deep arterial thrombosis in his leg. He didn’t want to use the CDS and now he is amazed by the results.”
Autoimmune and Inflammatory Skin Conditions
Now let’s take a look at some autoimmune and inflammatory skin conditions with explanations about potential mechanisms of action and also anecdotal testimonials. If the science bore you or is over your head, just skip down to the testimonials.
Autoimmune and inflammatory skin diseases share many of the same pathological themes described for diabetic foot ulcers: dysregulated redox balance, chronic innate and adaptive immune activation, microvascular dysfunction, impaired barrier repair, and microbial triggers or superinfection. Because chlorine dioxide and chlorite act primarily as redox‑active immune modulators and antimicrobials, many of the mechanisms proposed for ulcer healing plausibly overlap with mechanisms relevant to conditions such as psoriasis, atopic dermatitis, cutaneous lupus, and chronic eczematous or neutrophilic dermatoses.[4, 18]
Redox modulation and oxidative stress
Autoimmune and inflammatory skin disorders are frequently characterized by elevated reactive oxygen species (ROS), oxidative damage to lipids and proteins, and activation of redox‑sensitive inflammatory pathways (for example NF‑κB, inflammasomes, and cytokine cascades). Chlorite complexes (such as TCDO/WF10) have been shown to selectively reduce superoxide while increasing hydrogen peroxide in a range that favors endothelial and tissue repair functions, likely via increased superoxide dismutase (SOD) activity and altered myeloperoxidase activity. In skin disease, a similar shift could theoretically dampen oxidative injury to keratinocytes and endothelial cells, decrease redox‑driven activation of inflammatory signaling, and restore a more controlled ROS milieu that supports tissue remodeling rather than chronic damage.[4, 18, 19]
Macrophage polarization and innate immune tone
Many inflammatory skin diseases show an imbalance in macrophage polarization, with excessive pro‑inflammatory M1 macrophages and inadequate reparative M2 macrophages contributing to chronic inflammation and matrix breakdown. Chlorite (WF10/NP001) has been shown to down‑regulate pro‑inflammatory monocyte and macrophage genes, inhibit M1‑type activity, and promote conversion toward an anti‑inflammatory, wound‑healing phenotype, in part through generation of taurine chloramine via myeloperoxidase‑mediated reactions. In autoimmune or inflammatory skin disorders, this same mechanism could rebalance macrophage populations in lesional skin, reducing production of TNF, IL‑1, IL‑6 and other cytokines while enhancing phagocytosis and clearance of debris, thereby resolving chronic inflammation and facilitating repair. [4, 18, 20, 21, 22]
T‑cell activation and cytokine networks
Conditions like psoriasis, cutaneous lupus, and some eczematous disorders involve persistent activation of T cells and pathogenic cytokine loops (for example IL‑17/IL‑23, IL‑22, IFN‑γ), which drive keratinocyte hyperproliferation and tissue damage. In vitro and clinical data show that chlorite‑based formulations can suppress T‑cell proliferation, down‑regulate T‑cell activation markers (CD38, CD28, HLA‑DR), and reduce IL‑2 and other pro‑inflammatory mediators in peripheral blood mononuclear cells. Translating this to skin disease, such T‑cell dampening might help break the self‑amplifying cytokine circuits in psoriatic or autoimmune skin lesions, while the macrophage‑modulating effects could synergistically reduce the upstream antigen‑presenting and co‑stimulatory signals that maintain pathogenic T‑cell responses. [4, 23, 24, 25]
Neutrophil activity, chloramines, and resolution of inflammation
Neutrophils and their oxidative products (including hypochlorous acid and secondary chloramines) play dual roles in skin: essential antimicrobial defense but also drivers of tissue damage and chronic inflammation when unchecked. Chlorite‑based drugs can inhibit excessive polymorphonuclear cell migration and activation while promoting generation of taurine chloramine, a relatively mild, endogenous chloramine that delivers anti‑inflammatory signals and turns off NF‑κB in macrophages. In neutrophilic or auto‑inflammatory skin conditions (for example pustular psoriasis or some vasculitides), re‑shaping this neutrophil/chloramine axis might reduce destructive oxidative bursts and protease release, while preserving enough innate function to control microbes. [4, 18, 19, 20]
Microbiome, infection, and barrier integrity
Cutaneous microbiome imbalance and recurrent or subclinical infection often sustain or aggravate inflammatory skin diseases, especially when the barrier is impaired. Chlorine dioxide is a size‑selective oxidant that can rapidly inactivate bacteria, fungi, and viruses by oxidizing key amino acids and nucleic acids, with a track record as a potent but relatively tissue‑sparing topical antiseptic. In inflammatory dermatoses with secondary infection or biofilm formation, topical ClO₂ or related chlorite formulations could theoretically reduce microbial load and biofilm‑associated immune stimulation, while their immune‑modulating and redox‑balancing effects simultaneously support barrier repair and normalization of the local microbial ecosystem. [4, 19, 26, 27]
Microvascular function and tissue remodeling
Microvascular changes, including endothelial dysfunction, altered angiogenesis, and low‑grade ischemia, are described in several chronic inflammatory and autoimmune skin conditions. Chlorite complexes have been shown to increase tissue oxygen tension, enhance physiologic angiogenesis, and stimulate formation of granulation tissue and collagen in chronic ulcers, effects linked to optimized hydrogen peroxide signaling and SOD activity. In inflammatory skin disease, similar actions could improve dermal perfusion, oxygen delivery, and matrix remodeling, countering the fibroatrophy and scarring that often accompany long‑standing inflammation.[4, 18]
Integrated, overlapping mechanisms
Taken together, the mechanisms described for ulcer treatment—redox recalibration, macrophage and T‑cell modulation, controlled neutrophil activity and chloramine signaling, broad‑spectrum antimicrobial action, and improved microvascular‑tissue repair—map closely onto key pathological processes in autoimmune and inflammatory skin disorders. While direct clinical data in these diseases are limited, the convergence of pathways suggests that chlorine dioxide and chlorite‑based therapies could, in principle, shift diseased skin from a state of chronic immune over‑activation and oxidative injury toward one of controlled immunity, restored barrier function, and active repair, warranting formal exploratory and randomized studies in these indications. [4, 18, 20]
Testimonial: Hyperkeratosis Pustular Psoriasis

(Translated from Italian)
“Hyperkeratosis pustular psoriasis, healed in 3-4 months with protocol C plus maintenance and CDS + DMSO sprays. All associated with a carbohydrate-free diet. I attach photos as evidence and I thank the people who helped me and made this precious journey known.
Maurizio da Verona”
**editors note: The CDS and DMSO were in different spray bottles
Testimonial: Rash Unknown Cause

“Last Christmas I also got a rash on my body - I am not perfect, but I eat clean and I don’t use prescription drugs. I am a practitioner that works very closely with people who are detoxifying and this is the only thing I could figure out of why I had this rash. No one could help me- even my trusty medical ozone treatments and utilizing ozonated oil did not help. This was so difficult! I was up night after night and it itched- or it hurt- alternating. I took ivermectin and also used the paste on my skin. It helped bit- but it would not go away. I even went to a doctor- but they wanted steroids and antibiotics. And it was getting worse as well- trying to start around my neck and ankles. Doctor said: allergy… hives… they tested for MRSA, etc all to no avail. This was when I watched the Lindsay Wagner video that Curious Outlier had posted on Substack- and that was all I needed. It should be noted here that my experience here happened before the two above stories- this was my first time experimenting with using it- here’s my arms after about 10 days of trying everything I could think of- I was also down to eating carnivore- no carbs/caffeine, etc
I was wearing long sleeved shirts and I was utterly miserable. I followed the CDS stock solution but only used 8 drops of Part A and 12 drops of HCL (Part B) in 16 oz. I drank small amounts throughout the day with no negative reaction. I sprayed it on my arms as well- the spray included 3-4 drops of 70% DMSO with the CDS solution.
Within 3 days the changes were obvious. The doctor had told me to use antihistamines- I had tried them shortly but they made me tired. I stopped them and only stayed with the CDS/DMSO. My arms cleared up- itching stopped. My neck/ankles are fine. I now use CDS mixture at 20 drops Part A and 25 drops HCL (Part B) in 16 oz water for maintenance. I drink about a tbsp of my CDS stock mixture with one drop of DMSO in about 6 oz of water once every other day or every third day for maintenance. Here are my arms-
God is good!!! Thank you Curious Outlier- and Dr Andreas Kalcker! Dr Pierre Kory as well, as a natural health practitioner for over 20 years I have learned such incredibly important information through you all and I am still learning. I am a 20+ year survivor of breast cancer (no chemo/radiation) and I have recovered from fibromyalgia, CFS (chronic fatigue syndrome), MS and Lupus. I am 66 and am thankful for every day of my miraculous life.”
Protocols Used:
Spray protocol + DMSO
Testimonial:

“Hello dear Massimo! I thank you from the bottom no of my heart for the advice and the help you have given me!!!🤗 I am following your advice and the protocol for the treatment of psoriasis and it has been working slowly. You can see the results even after just 15 days. It is in a very advanced form and it takes time. Today is now 22 days since I have been taking and spraying cds and dmso on my palmoplantar psoriasis. I am sending you photos, the first two are before starting, swollen insoles and with deep ulcers, I had become an invalid. My husband assisted me with everything. I could not even stand up!😭
(Translated from Italian)
Today is the 22nd day and it is gone, my feet don’t hurt and I can walk without any problems: God Bless you!!!!
To you and your whole family!!! You know, taking cds and dmso I’m noticing that my memory is also improving”
‼️➡️Need more info? Click to ask questions.
Testimonial: Chronic Psoriasis

“Psoriasis for over 15 years with this, but with CD-S, disinfection...in recovery !!”
Protocol used: Protocol D (spray protocol)
Testimonial: Chronic Psoriasis

“38-year-old man, with psoriasis since he was 16 years old. Treatment with DMSO in a spray bottle, (because it was in many parts of the body) after CDS 50% and 50% water. Result in less than 30 days, and taking CDS protocol C until now.”
Testimonial: Eczema

Kalcker method was used to make CDS but only one round for 1/2 strength approx 1500 ppm. The parent dipped their finger in the CDS1500 and dabbed in on the affected areas 2 x per day.
Testimonial: Chronic Dermatitis

“This 55 year old woman had atopic dermatitis since adolescence. She had little response to conventional and alternative treatments for 30 years until she tried the following:
Oral MMS for 3 months (Protocol B)
Topical spray several times a day with CDS (Protocol D)
Hot water bath with CDS (Protocol L)
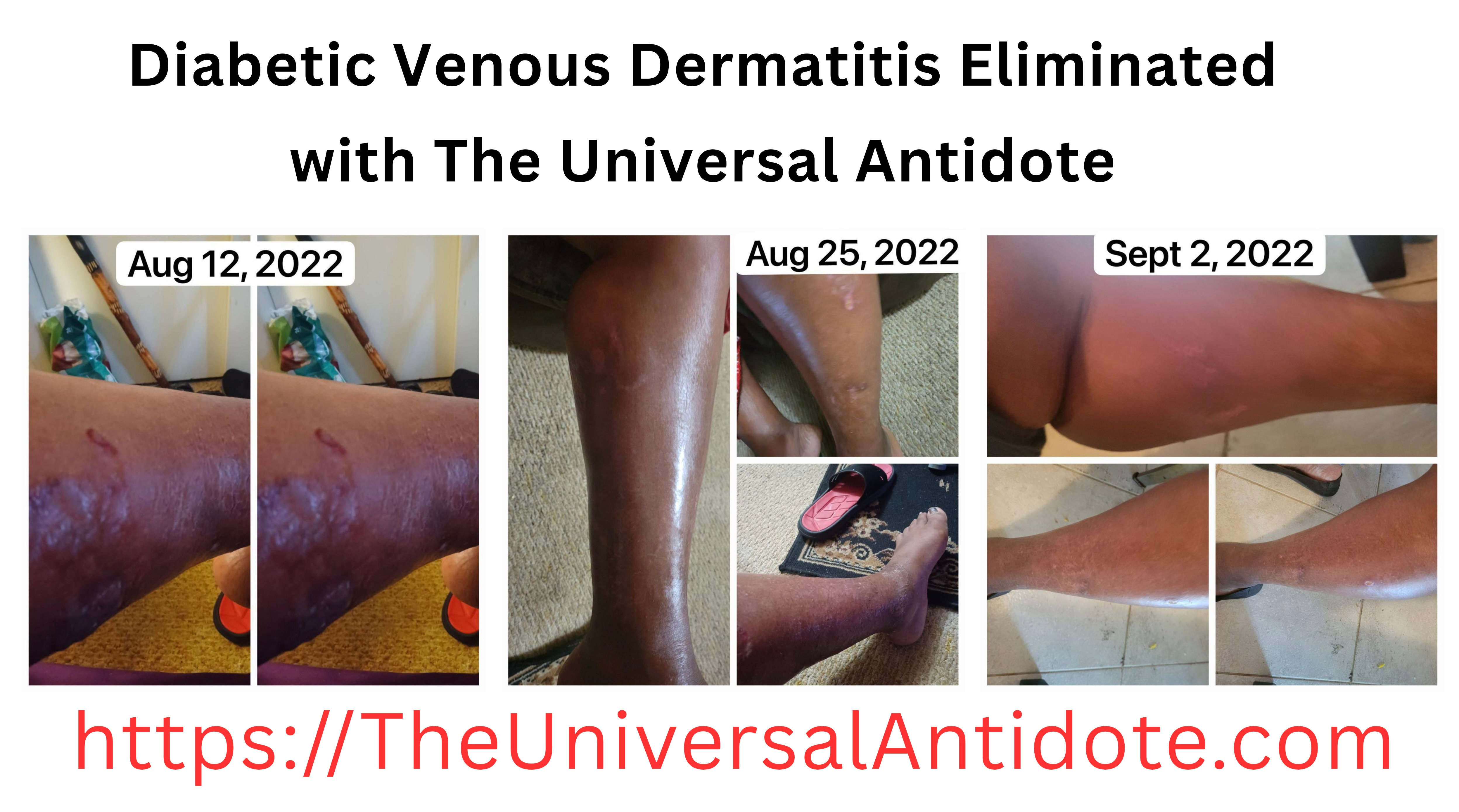
Testimonial: Diabetic Venous Dermatitis
To learn how to eliminate disease with join the private chat group here: https://bit.ly/JoinUniversalAntidotePrivateChat
First Set of 2 Pictures:
“Aug 12th 2022 this is my mom age 73 with no MMS yet.”
Second Set of 3 Pictures:
“Aug 25 2022 she only spraying with the MMS Spray Bottle Protocol, she’s not taking MMS1 internally yet. Shes diabetic and they’re trying to put her in the hospital.”
Third Set of 3 Pictures:
“September 2 2022 She Just started taking MMS1 internally on Wednesday Aug 31st.”
Testimonial: Chronic Dermatitis
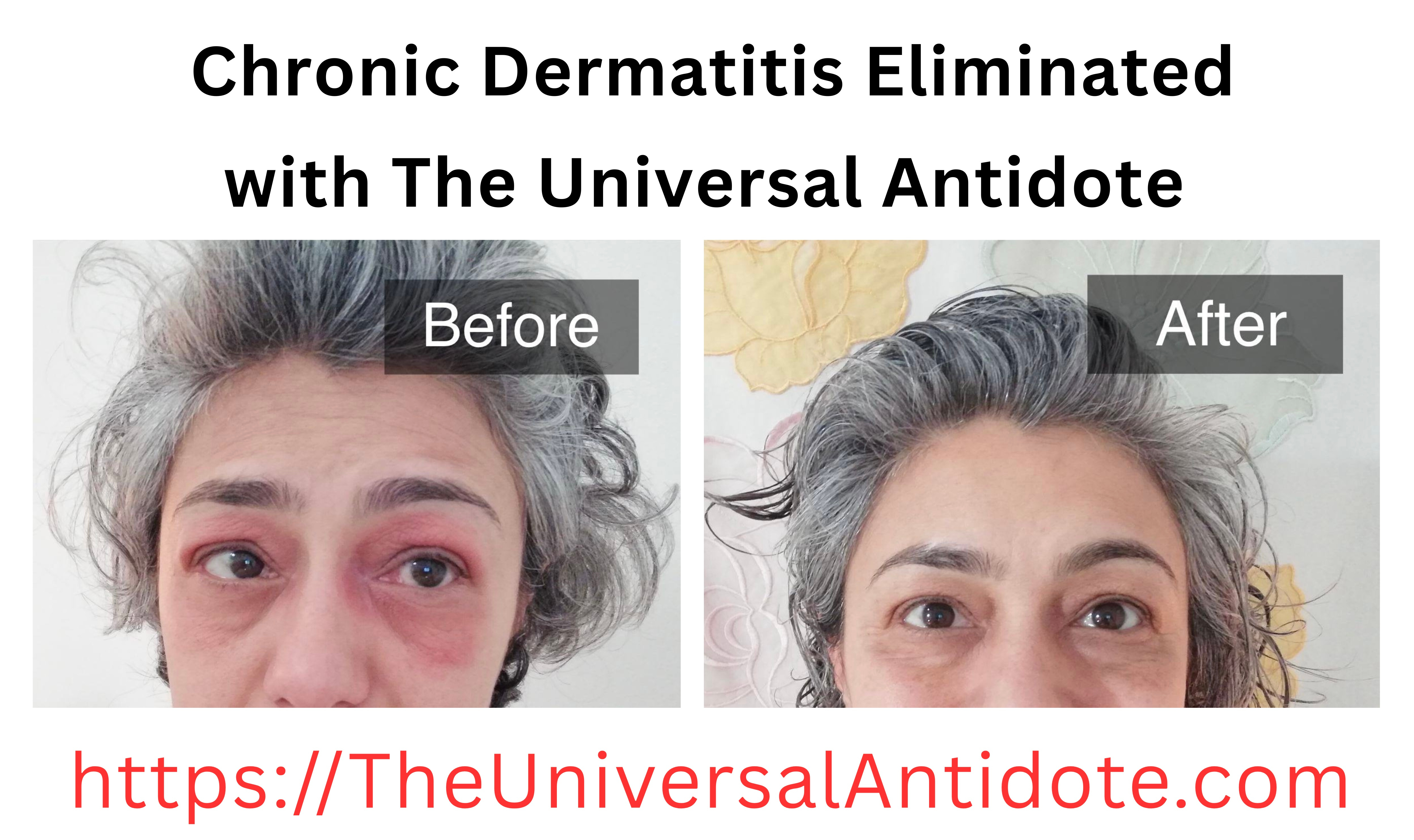
(Translated from Italian)
“I had dermatitis on one eye for 5 months that also spread to the other: itching, flaking, red spots, and skin full of wrinkles all around the eyes.
Out of a rush to heal, I misused CDS, spraying it every hour without diluting it.
Instead, on Nazarena’s advice, I diluted it 50% with Lauretana water and sprayed it “only” 3 times a day, covering it for a few minutes to prevent evaporation and then applying pure aloe vera gel. The results were incredible and immediate in just 5 days.
Thank you so much!
Now I know I can recommend and promote CDS!”
Testimonial: Psoriasis

Protocol used: Protocol D
Testimonial: Age Spots Fading

(Translated from German)
A 70-year-old man used homemade CDS (Sealed Jar method) with measured ~2500ppm.
After 4 weeks of spraying morning and evening on the scalp, the pigment spots have faded.
He was visibly delighted and also enjoys a cooling effect with the CDL spray on warm summer days.
Protocol Used: Protocol D
Testimonial: Chronic Neurodermatitis

(Translated from German)
“Hi everyone.
I used CDS for several months and after 50 years of neurodermatitis I had great success with it. My gratitude brought me here to encourage other neurodermatitis patients to try it out.
First I drank CDS, which didn’t do much for my skin.
Then I sprayed it directly onto the skin using a small spray bottle (dm) in a 1:1 ratio. (3 times a day.)”
Other Skin Problems
The chlorine dioxide spray protocol has proven highly effective for a variety of skin conditions, though I can’t always fully explain the mechanisms behind its success. Some conditions, like acne, are easier to understand since the mechanisms likely align with those discussed earlier in this article. Others—such as urticaria and keratosis—are less clear, yet the results remain consistent. I’ve also observed that chlorine dioxide can quickly stop reactions from poison ivy or chemical irritants on the skin. While the precise mechanisms of action for some of these effects are still uncertain, experience has shown that the spray protocol often works remarkably well, even without a complete scientific explanation. My motto is, “My motto is “it sure can't hurt to try it.”
Testimonial: Possibly Seborrheic Keratosis or Pigmented Nevi
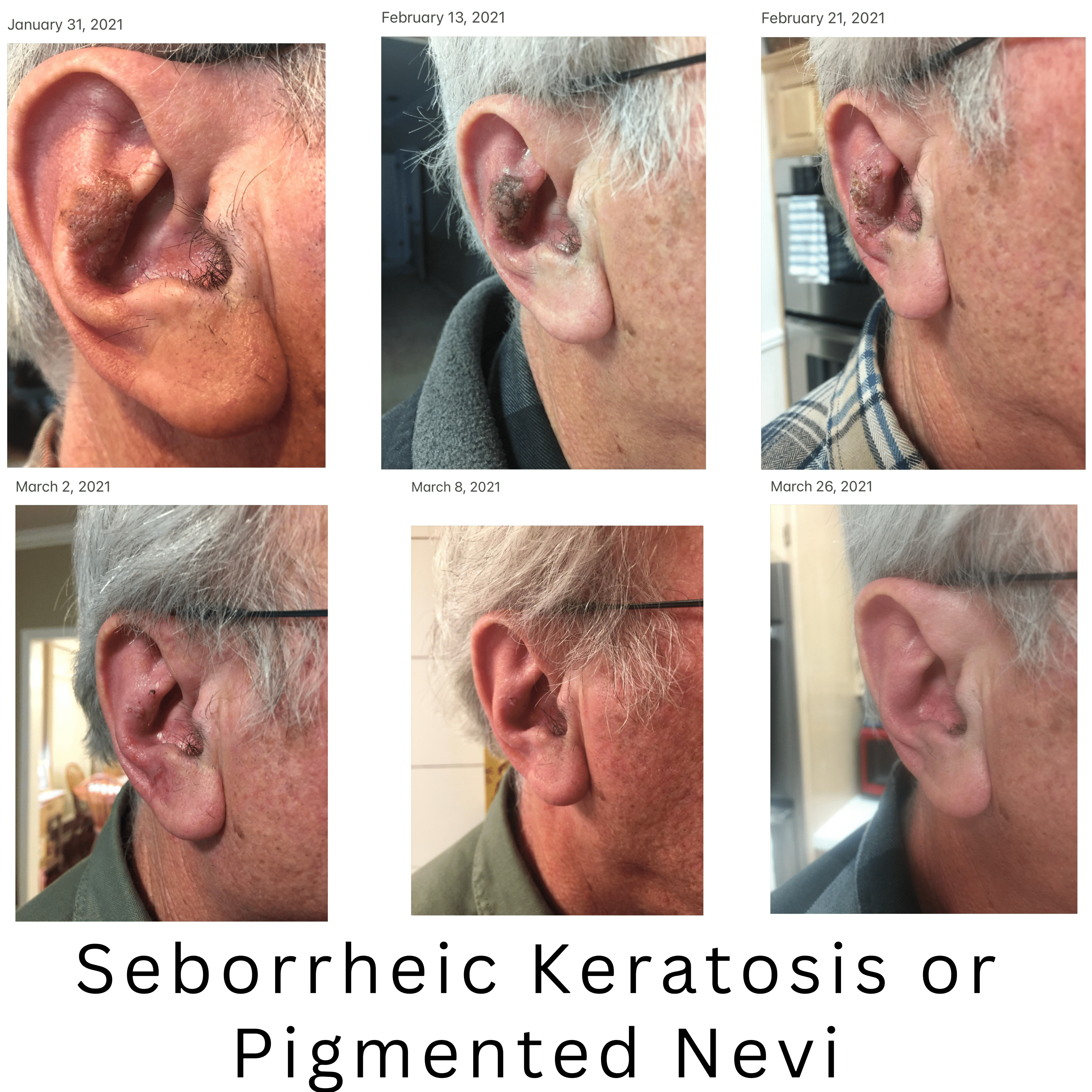
The spray protocol was used and he applied a drop of DMSO to the area a few minutes before the application of the chlorine dioxide spray.
Applied twice per day for approx.
The lesion was eliminated in 55 days.
Testimonial: Seborrheic Keratosis

(Translated from Italian)
Message 1
“Good morning I leave my testimony, my sister, I advised her to try to spray the cds and pure several times a day, this is the result. Have a good day everyone.”
Message 2
“I would like to point out that my sister is 61 years old and in fact, as you can see from the photos, the small skin tags that she also had on both her breasts and her neck have also gone away. She put on hi the CDS and then DMSO morning and evening for 3 weeks. In the other message I forgot to say that she used both products, just be careful because in the middle of the breast (for those with large breasts) the CDS initially caused problems because she wasn’t breathing and, by blocking, created redness. So she waited lying down for a moment for it to dry.
Protocol Used: PROTOCOL K
Testimonial: Poison Ivy

POISON IVY PROTOCOL
Spray CDS 3000 topically every 15 minutes to affected areas till resolved.
Testimonial: Acne

(Translated from Spanish)
“This is how his skin improved in less than 2 months of applying Chlorine Dioxide with spray, (she didn’t even take it). She left the treatment of her Dermatologist.”
Testimonial: Acne

(Translated from Spanish)
*Hello, I want to share my testimony about ACNE*
My acne started when I was 12 years old. Since then, it’s been super inflammatory, mostly on my cheeks and around my lips. It was so aggressive that my face looked swollen until I went to a general practitioner, and he prescribed a topical oral treatment. My acne improved, was no longer as inflammatory, and my face no longer looked swollen. But my continuous acne was not completely cured, years went by and I continued to break out. At 17, it became inflammatory again but not as severe, but there were a lot of breakouts on my cheeks, forehead, around my lips and temples. My acne continued for years until 2019 when I learned about CDS and DMSO but I didn’t have faith in it so I only used it twice and it dried out the breakout, but I didn’t continue using it and until 2022 I decided to use the topical protocol well, which is CDS, DMSO and again CDS in sprite everything and it was what made my acne disappear and improve a lot! I’m attaching photos of what my skin looks like today and photos from the past ✨
Also, I want to mention that the 11 years my acne continued, and it did a lot of damage to my skin, leaving me with many scars, like pits or ice picks. I also added the psychological trauma it left me with, and I’m still treating them to this day because it greatly affects my self-esteem. But I’m very grateful that the outbreak is no longer common on my skin. I admit I still have to follow the protocols taking it to fully cure it, but topically, I’ve already treated it and it worked very well for me. ✨”
Testimonial: Acne

Testimonial: Acne

(Translated from Spanish)
My daughter before and after applying chlorine dioxide on her face, 1 milliliter of CDS in 10 milliliters of water, applied morning, afternoon, and night with a spray bottle.”
Testimonial: Brown Recluse Spider Bite

(Translated from Italian)
“Brown recuse spider bite, after a few days of antibiotic which was not giving the desired results I decided to apply CDS and Dmso, in a 30 ml dark glass bottle I put 20 drops of Dmso and 25 ml of CDS, sprayed directly on the injured area, the first week once every two hours then 3 times a day, these are the results in 10 days of treatment”
Testimonial: Severe Burn
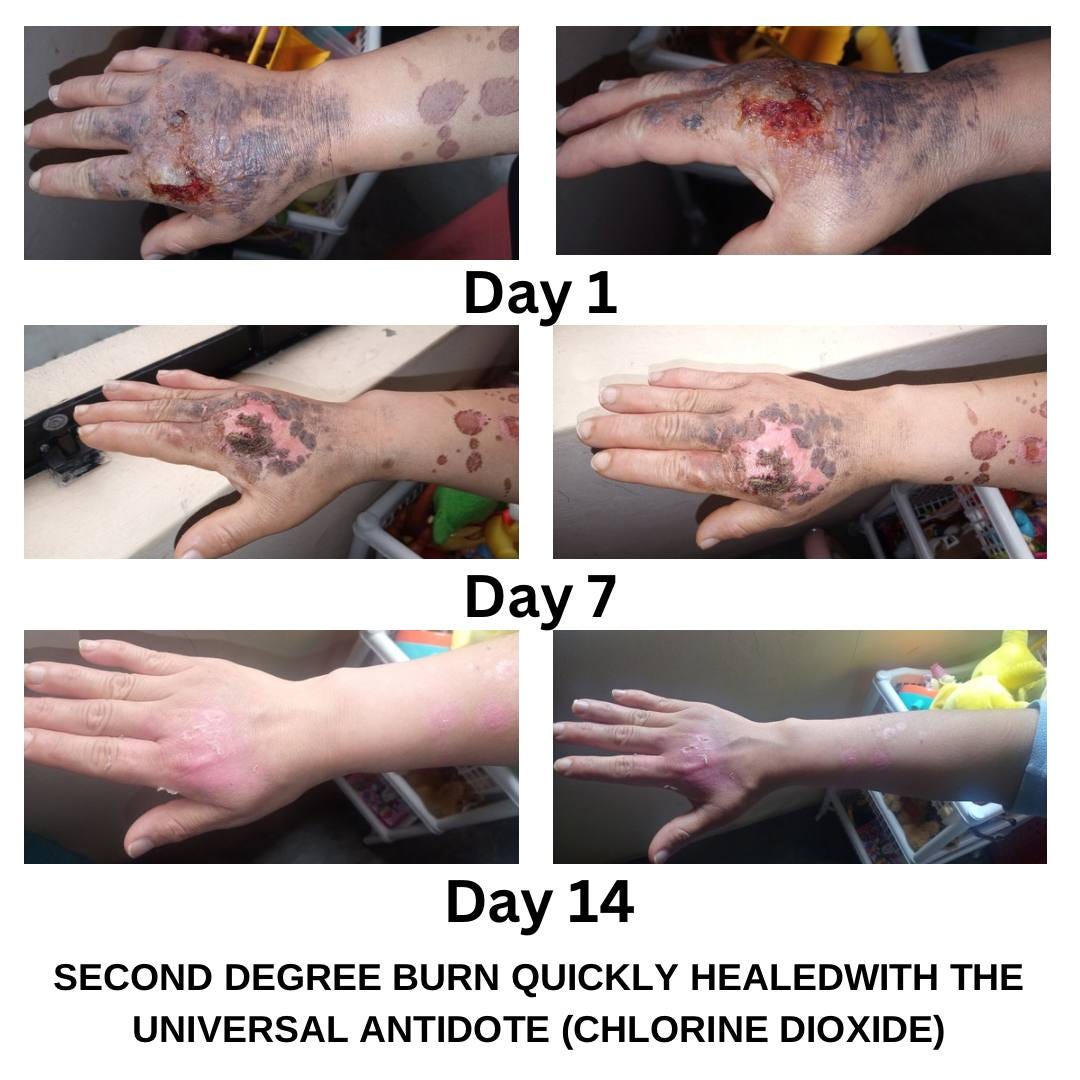
“First day of applying CDS spray and Protocol C, second-degree burn from cooking oil.
Second photo taken 7 days after applying CDS spray at 10 ml per liter.
Third photo taken 14 days after applying CDS spray and Protocol C, the burn almost imperceptible.”
Testimonial: Severe Burn

“Follow-up of skin regeneration after heat-induced eyelid burn. (A): Lesion on day zero of treatment; (B): Lesion on day 2 of treatment; (C): Lesion on day 4 of treatment; (D): Lesion on day 14 of treatment; (E): Lesion on day 22 of treatment.
On December 7, 2021, a 15-year-old male with Down syndrome and astigmatism, suffered a burn from sudden exposure to the flame of a water heater, which affected the skin area on his upper and lower eyelids. The skin lesion was diagnosed as a second-degree burn caused by physical heat. Prior to antiseptic therapy with CD, the eye was treated for the first 48 hours with Besifloxacin 0.6% ophthalmic suspension every 8 h and a Tobramycin/dexamethasone ointment (3mg/1mg/g) every 12 h, as recommended by another physician. After 48 h, the antibiotic treatment was suspended and on December 9, 2021, treatment with CD began. The first day of CD treatment consisted of three F15 protocols (30ml CD at 3,000 ppm diluted in 1L of H2O) taken orally every 3 h until finishing the liter, and on the application of protocol D (CD at 3,000 ppm diluted 1:3 in 0.9% NaCl) over the lesion every 2-3 h. The second day of treatment was a C20 protocol (20ml CD at 3,000 ppm diluted in 1L of H2O) taken orally every hour during 10 h until finishing the liter, and the application of protocol D to the lesion every 2-3 h. Between days 3 to 7 of treatment, a C20 protocol was taken, protocol D was applied and an ophthalmic suspension was added according to protocol O (5ml CD at 3,000 ppm diluted in 50ml of 0.9% NaCl with 3ml of dimethyl sulfoxide, DMSO, at 70%) every 3-4 h. Between days 8 to 18 of the CD treatment, protocol D and O were followed.”
👉 Find the study on the Internet
Testimonial: Severe wounds from dog bite

“Hey guys. I want to share my improvment to show how great is MMS and to give hope for anyone struggling.
I was bitten violently by a husky dog on June 25th. 25stitches were kept in and extracted after 1 week.. my wounds were deep close to my mouth and chin area. Cosmetic clinics would have me injected with toxic steroids and use CO2 fractional laser with resurfacing... Normally the face area needs 1-2years of healing time....
Ofc I refused to do that and came across MMS only in August with a super long shipping time so I could start the spray protocol + low and slow working up my way to protocol 1000....Even tho the collagen started forming and the epidermis layer was already very much active, MMS still helped and helps me a lot...I’m 3 months and 1 week after the accident.”
References:
UHNM, et al. A systematic review on chlorine dioxide as a disinfectant. J Med Life. 2022 Mar;15(3):313-318. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9015185/
Wang SS, et al. Efficacy and Safety Evaluation of a Chlorine Dioxide Solution. Int J Environ Res Public Health. 2017 Mar 22;14(3):329. https://pmc.ncbi.nlm.nih.gov/articles/PMC5369164/
Helou M, et al. Antimicrobial effects of chlorine dioxide in a hospital setting. Sci Rep. 2023 Dec 18;13(1):22866. https://pmc.ncbi.nlm.nih.gov/articles/PMC10739700/
Calliperis, P., et al (2024). Chlorine dioxide and chlorite as treatments for diabetic foot ulcers. International Journal of Medicine and Medical Sciences, 16(1), 1–14. https://doi.org/10.5897/IJMMS2023.1503
Callisperis, P., et al (2024). Chlorine dioxide treatment for diabetic foot ulcers: Three case studies. International Journal of Medicine and Medical Sciences, 16(2), 44–49. https://doi.org/10.5897/IJMMS2024.1515
Maraprygsavan P, et al. The chlorite‑based drug WF10 constantly reduces hemoglobin A1c values and improves glucose control in diabetes patients with severe foot syndrome. Journal of Clinical and Translational Endocrinology. 2016. https://www.sciencedirect.com/science/article/pii/S2214623716300072
Yingsakmongkol N, Maraprygsavan P, Sukosit P. Effect of WF10 immunokine on diabetic foot ulcer therapy: a double‑blind, randomized, placebo‑controlled trial. The Journal of Foot and Ankle Surgery. 2011. https://www.sciencedirect.com/science/article/abs/pii/S1067251611002560
Yingsakmongkol N, et al. Effect of the chlorite‑based drug WF10 on hemoglobin A1c and hematological biomarkers in uncontrolled diabetic patients with foot ulcer. Journal of Diabetes and Treatment. 2021. https://www.gavinpublishers.com/article/view/effect-of-the-chlorite-based-drug-wf10-on-hemoglobin-a1c-hematological-biomarkers-in-uncontrolled-diabetic-patients-with-foot-ulcer
Tissot M, et al. Anti‑inflammatory properties of a novel wound‑healing and immunomodulating agent, tetrachlorodecaoxygen complex (TCDO). Agents and Actions. 1990. https://link.springer.com/article/10.1007/BF01997633
Giese T, et al. Differential effects on innate versus adaptive immune responses by WF10. Cellular Immunology. 2004. https://www.sciencedirect.com/science/article/abs/pii/S0008874904001315
Schönberg M, Schlorke D, Arnhold J. Effects of WF10 on glycosaminoglycan sulphation in proinflammatory monocytes and macrophages. In: Flow Cytometry – Select Topics. 2016. https://www.intechopen.com/chapters/49202
Miller RG, et al. NP001 regulation of macrophage activation markers in ALS: a phase I clinical and biomarker study. Amyotroph Lateral Scler Frontotemporal Degener. 2014 Dec;15(7-8):601-9. https://pmc.ncbi.nlm.nih.gov/articles/PMC5524125/
Benarde MA, et al. Efficiency of chlorine dioxide as a bactericide. Appl Microbiol. 1965 Sep;13(5):776-80. https://pmc.ncbi.nlm.nih.gov/articles/PMC1058342/
Alvarez ME, O’Brien RT. Mechanisms of inactivation of poliovirus by chlorine dioxide and iodine. Appl Environ Microbiol. 1982 Nov;44(5):1064-71. https://pmc.ncbi.nlm.nih.gov/articles/PMC242149/
Sanekata T, et al. Evaluation of the antiviral activity of chlorine dioxide and sodium hypochlorite against feline calicivirus, human influenza virus, measles virus, canine distemper virus, human herpesvirus, human adenovirus, canine adenovirus and canine parvovirus. Biocontrol Sci. 2010 Jun;15(2):45-9. https://www.jstage.jst.go.jp/article/bio/15/2/15_2_45/_pdf/-char/en
Al-Bayaty F, Abdulla MA. A comparison of wound healing rate following treatment with aftamed and chlorine dioxide gels in streptozotocin-induced diabetic rats. Evid Based Complement Alternat Med. 2012;2012:468764. doi: 10.1155/2012/468764. Epub 2012 May 15. Erratum in: Evid Based Complement Alternat Med. 2019 Jan 10;2019:4265081. https://pmc.ncbi.nlm.nih.gov/articles/PMC3362038/
Hinz J, Kühne FW, Stahl KW. Local tetrachlorodecaoxide treatment to improve oxygen supply to non-healing wounds. Lancet. 1984 Sep 15;2(8403):630. https://www.jpsmjournal.com/article/S0885-3924(97)00018-3/pdf
Xia T, et al. Advances in the study of macrophage polarization in inflammatory immune skin diseases. J Inflamm (Lond). 2023 Oct 12;20(1):33. https://pmc.ncbi.nlm.nih.gov/articles/PMC10568804/
Snell JA, Jandova J, Wondrak GT. Hypochlorous Acid: From Innate Immune Factor and Environmental Toxicant to Chemopreventive Agent Targeting Solar UV-Induced Skin Cancer. Front Oncol. 2022 Apr 29;12:887220. https://pmc.ncbi.nlm.nih.gov/articles/PMC9106365/
Zhang R, et al. Macrophage-Targeted Sodium Chlorite (NP001) Slows Progression of Amyotrophic Lateral Sclerosis (ALS) through Regulation of Microbial Translocation. Biomedicines. 2022 Nov 12;10(11):2907. https://pmc.ncbi.nlm.nih.gov/articles/PMC9687998/
S, Kawamoto M, et al. M1/M2 Macrophage Skewing is Related to Reduction in Types I, V, and VI Collagens with Aging in Sun-Exposed Human Skin. JID Innov. 2023 Aug 12;3(6):100222. https://pmc.ncbi.nlm.nih.gov/articles/PMC10542643/
Yunna C, et al. Macrophage M1/M2 polarization. Eur J Pharmacol. 2020 Jun 15;877:173090. https://www.sciencedirect.com/science/article/abs/pii/S0014299920301825
Khalid SI, et al. Immune Modulation in the Treatment of Amyotrophic Lateral Sclerosis: A Review of Clinical Trials. Front Neurol. 2017 Sep 25;8:486. https://pmc.ncbi.nlm.nih.gov/articles/PMC5622209/
Wang Y, et al. Tripterygium wilfordii Hook. F. and Its Extracts for Psoriasis: Efficacy and Mechanism. Drug Des Devel Ther. 2023 Dec 20;17:3767-3781. https://pmc.ncbi.nlm.nih.gov/articles/PMC10749103/
Li C, et al. Psoriasis-associated impairment of CCL27/CCR10-derived regulation leads to IL-17A/IL-22-producing skin T-cell overactivation. J Allergy Clin Immunol. 2021 Feb;147(2):759-763.e9. https://pmc.ncbi.nlm.nih.gov/articles/PMC7726097/
Gottardi W, et al. N-chloramines, a promising class of well-tolerated topical anti-infectives. Antimicrob Agents Chemother. 2013 Mar;57(3):1107-14. https://pmc.ncbi.nlm.nih.gov/articles/PMC3591902/
Aparicio-Alonso, M. (2022). Infection prevention and tissue repair in skin lesions using treatments based on a chlorine dioxide solution: Case studies [Preprint]. Authorea. https://www.authorea.com/users/568645/articles/614420-infection-prevention-and-tissue-repair-in-skin-lesions-using-treatments-based-on-a-chlorine-dioxide-solution-case-studies